With no day shelter available, unhoused persons find themselves without a “place to be”
By Nancy English
John Friedman-Gruber was homeless, is now housed, and is overflowing with gratitude for those who helped him. Especially, “Another person who was and is I believe an angel. Her name is Gretchen [Bisco]. She works for the city and if it wasn’t for her, I’d probably be dead.” He emailed me after reading the May article about homelessness in the West End News.
He wrote that he hoped, “My words might encourage maybe at least one person to get out – to show that they can do it as well.”
“They need a place to be.”
Gretchen Bisco is a housing navigator for Portland. Just like her, there are many, many people ready to help. But limited resources at every step frustrate all involved.
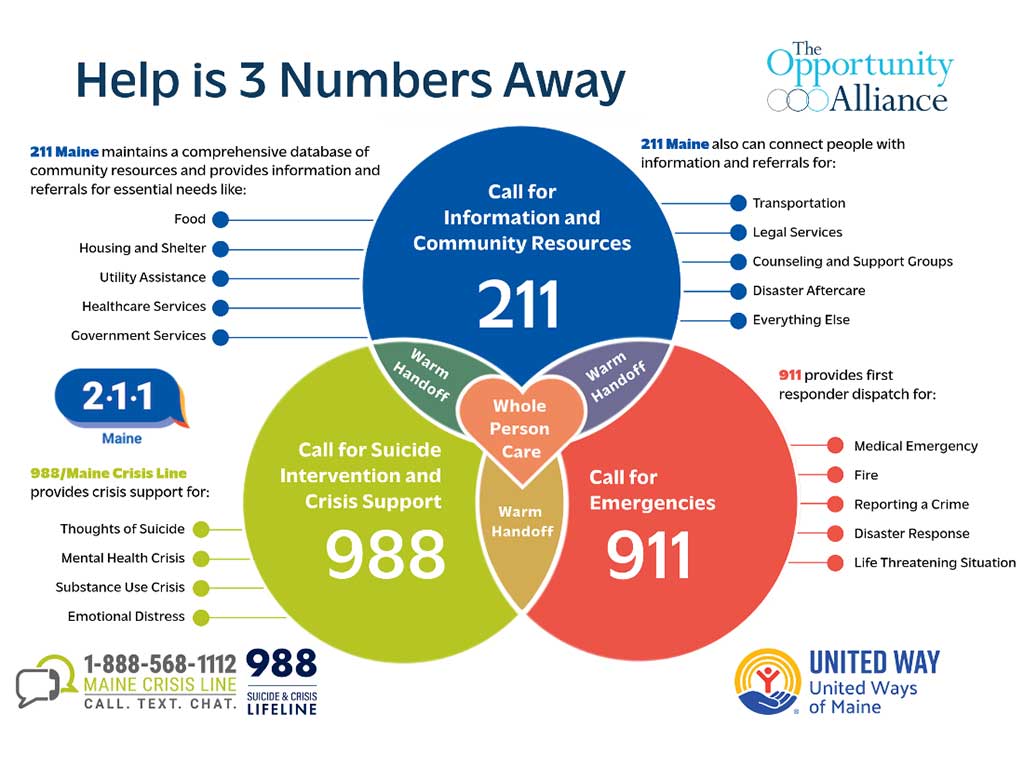
The people answering phones at the Crisis Prevention Line, statewide 1-888-568-1112 (or 988), are champions for the homeless and the mentally ill. Opportunity Alliance runs Cumberland County Crisis Response, with an average of 300 contacts a month and a mobile team that goes to clients. Director Carrie Swarthout has eight years of experience in this program.
For a person dealing with a mental health crisis, “A place to be is the first need,” Swarthout said. “Most wait for a group home for a year. First, they must be connected to a counselor, and a case manager,” and have basic needs met. Crisis Prevention Services calls shelters hoping to find a temporary “place to be.” But there is no daytime destination.
The Behavioral Health Unit of the Portland Police Department has been responding to around 236 calls per month. Portland Police Dispatch workers send Behavioral Health staff to possible overdoses and to public and private reports of distress.

Supervisor Bridgit Sliwak began her role in Portland in 2016 with grant funding. Six people now work in PPD’s Behavioral Health group, funded in the annual city budget.
“It’s a lot of work to get better,” she said about her clients.
Many just need a place to go – again, there is no day space organized for homeless people in Portland. Without that, “sometimes we need to accept our discomfort,” when witnessing homeless unable to care for themselves, Sliwak said. “Everyone is working with a different level of trauma.”
“We need longer term support.”
If a person is found suffering from incapacitating mental illness and is considered a danger to themselves or others, the Portland police or a crisis prevention worker may bring them to the Maine Medical Emergency Department for an evaluation.
“A person may be in the emergency department for days,” Sliwak said, waiting for a bed in a Maine Health psychiatric unit like Spring Harbor.
Dr. James P. Wolak is a hospital-based psychiatrist and Senior Medical Director at Maine Health, with ten years working in an Emergency Department (ED). He said the average wait for a psychiatric bed in the Maine Health system is two days, but it can be longer in Maine Medical Center’s ED.
His focus is on issues that arise after release. “What we need” he said, “are the right supports after they leave the hospital…To really stop the cycling, we need longer term community supports,” including different levels of support in group homes.
“There were more state resources,” he said, “and they have dried up… There are patients in all MaineHealth facilities waiting for beds in supportive housing, who cannot be discharged.”
Some need acute psychiatric care at Riverview Psychiatric Center in Augusta, which has 92 beds. Many are occupied by the criminally insane or people in custody needing evaluation for competency, which leaves even fewer available for those with severe mental illness not in the criminal justice system.
Blue, White, and Green Papers
Blue, white, and green papers name court-ordered actions for persons whose mental illness first requires involuntary hospitalization. Wolak said many patients are willing to consent to mental health treatment when a diagnosis requiring hospitalization is shared with them, when they are found at risk of serious harm to themselves or others, or “face a reasonable certainty that they will suffer harm,” from lack of self-care, for example.
“The law is very strict here because we are balancing civil liberties with mental health care,” Wolak said. A blue paper, with a judge’s order for hospitalization, is an emergency response to an acute crisis. Most hospitalizations are voluntary, but involuntary commitments are “not rare,” Wolak said.
Within 72 hours of the judge’s order, a hospital must either discharge – which Wolak said is rare – seek voluntary commitment, or file a petition with the court for involuntary commitment or a “white paper” hearing with the patient present, involving a court-appointed attorney for the patient and an independent examiner. Because of the local district court schedule, this can take more than 72 hours, Wolak said.
A Progressive Treatment Plan (PTP), also called a “green paper,” applies to out-patient treatment only. Police can bring a patient out of compliance with a PTP to an emergency room for evaluation if they find evidence of a risk of harm to self or others, but not otherwise.
The legal, law enforcement, and mental health systems struggle to respond to individuals who are homeless. Meanwhile, the homeless have no dedicated place to go. “It is your right to live sick, if you want to,” Swarthout said.